

Dr Daniel Crespi
What's in a stool sample?

What's in a stool sample?
Call to Book an appointment at Royal Free clinic
Poo...it comes out of all of our kids and us (and if it doesn't you should come and see me!) but it can vary so much in its consistency and appearance.
What is normal, what gives it its colour (or colours) and what do the different consistencies mean?
As a paediatric gastroenterologist it has become so normal for me to openly discuss poo with my patients and families, that I can sometimes forget (until my kids remind me!) that for some it is still an awkward topic to discuss.
When I asked some parent's recently what topics they would like to know more about with regard to their children's digestive health, some of the replies were about poo and its consistency and colour.
So I've put together a simple guide about what is and what isn't normal poo in babies and children for parents. It covers the basics and is not exhaustive in its approach. Always remember though that if you have concerns about your child, you should seek medical attention regardless of what you read below, as this is only meant to be a helpful basic guide to this topic.
WARNING!!:
Be prepared for a few food related references when it comes to descriptions...seems to be the way with us medics.
Poo frequency -How often should my child poo?
In the beginning...
Most babies born at term will pass their first poo or Meconium (a thick dark tar like) poo within the first 48 hours of life. Delays greater than 48 hours may be a sign of a problem such as Hirschsprung's disease
where the bowel's nervous system hasn't developed fully leading to a bowel obstruction. There may be other symptoms including a swollen or distended belly, green/bile stained vomiting and even blood-stained diarrhoea. Feeding may be off and there may also be concerns about growth. Occasionally it presents later in life with really difficult to treat constipation in an older child.
As a rough guide....
Breast fed babies can poo as often as with every breast feed or just once a week! The consistency and colour is often described as mustard-like with seeds.
Formula fed infants generally poo less often than their breast fed compatriots and the consistency is a little firmer, more peanut-butter like ( I did warn you...!)
As children get older, their bowel habits and frequency of pooing is similar to adults. Even we (adults) can vary widely with our bowel habits, from 3 times a week to 3 times a day! This often comes as a surprise to families when I mention this in clinic.
An important point to note is that constipation is not defined only by the frequency or infrequency of bowel movements. Other symptoms such as pain, straining, accidental leakage, signs of stool witholding all need to be considered as well. The bowel habits of your child will change over time and in the first year of life may change in the first few months, with milk changes or when moving over to solid foods.
The whole picture of your child and their health, including growth patterns, needs to be considered rather than just one aspect when assessing bowel function.
Poo colour - What colour should my child's Poo be ?
The colour of poo is influenced by what we eat but is mostly derived from pigments. These organic pigments (bilins) come from the breakdown of the haem protein found within red blood cells as they get recycled towards the end of their lifespan. The pigments include biliverdin and bilirubin (the pigment that causes jaundice) and eventually end up as stercobilin. Now from the distant memory of a non-linguist verde means green and sterco refers to droppings or dung!
What are normal poo colours?
Generally anything green
and various shades of brown are normal.
Just a note about Yellow
poo - if poo appears excessively fatty, is difficult to flush away and quite stinky, then this may indicate a problem with fat maldigestion/absorption and should be evaluated.
Colours to be concerned about
include :
Red
or black
These colours may indicate bleeding from the gastrointestinal tract.
Bright red
blood usually indicates fresh bleeding from a source closer to the exit or even just around the exit - a small fissure or tear in the skin around the bottom after a hard poo has been passed for example is a common cause.
Black
stools can indicate blood that has had time to be digested by gut enzymes, so usually the source of bleeding is higher up the digestive tract. The poo passed is known as melaena and often has a tar-like appearance with a characteristic smell. It should always be evaluated thoroughly by a specialist.
This is unless of course you've recently had red food colouring / beetroot or are taking iron tablets (cause poo to turn black) etc. If your bowel habit is a little on the infrequent side, it can come as quite a surprise to see red/purple coloured toilet water/poo a couple of days after eating beetroot !
White or Clay
The other colour or lack of colour I should say, to cause concern, is when the stools are very pale and have a white or clay like appearance
-this can indicate that the bile pigments produced in the liver aren't passing through the bile pipework easily. They can't reach the gut so the stool produced has no colour.
An example of this may be in a newborn infant who develops jaundice after a few days and that doesn't fade away. Prolonged jaundice in a newborn (for two weeks in a term baby or 3 weeks in a baby born prematurely) and in whom the poo is very pale...needs to be evaluated thoroughly as this may indicate a condition known as biliary atresia. This needs to be promptly diagnosed and treated.
That's why part of the clinical examination of a jaundiced baby should ALWAYS include having a look at a poo sample.
Poo consistency - How hard or soft should my child's poo be?
Poo consistency reflects the time spent travelling through the large intestine or colon. One of the main functions of this organ is to reabsorb water from faeces, so that the final poo passed is solid and smooth.
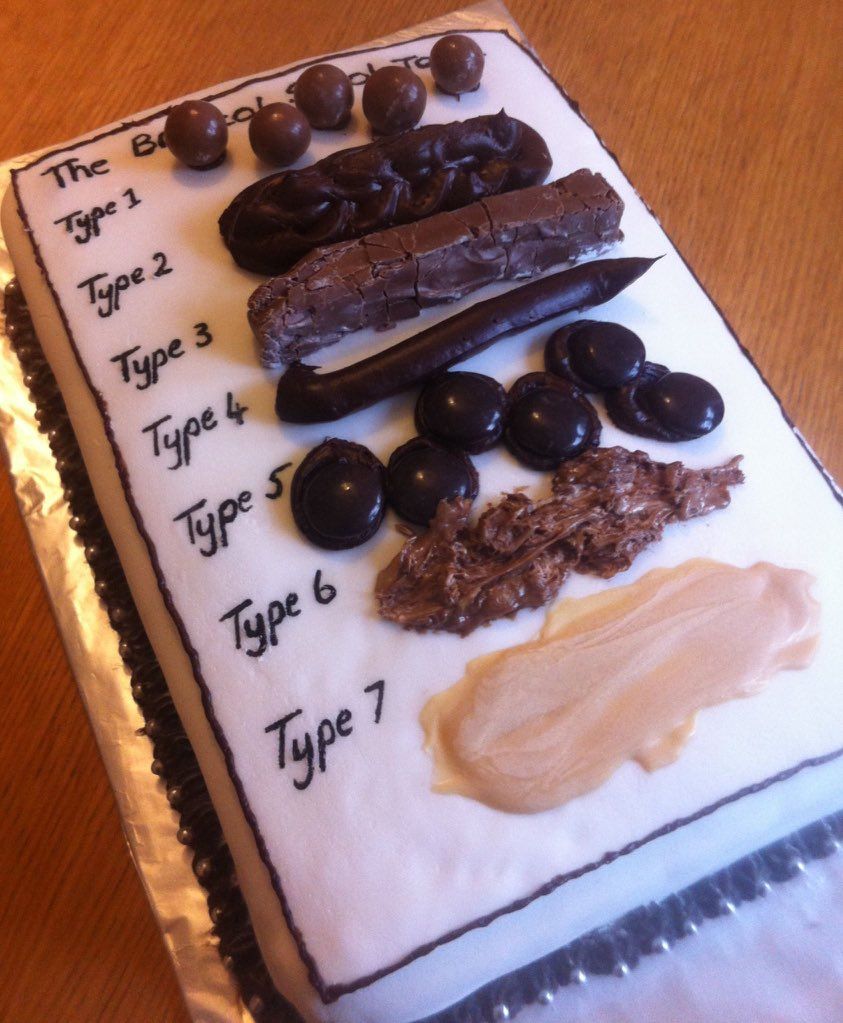
Poo researchers have studied the effect of bowel transit time on the consistency of poo and have produced charts such as the Bristol stool chart. This has 7 different stool consistencies 1 to 7. I even walk around with one in my clinic !! I find that it is sometimes a lot easier to use a chart when asking for a description of poo, than relying on words. It can also often make for a light hearted-moment in clinic.
The longer a poo resides in the bowel before exit, the more water is absorbed from it leaving harder type 1, 2 or 3 stool consistency. Poo that leaves the bowel in a hurry is more type 6 or 7.
Ideally we should see type 4 (a smooth slippery sausage like poo) being passed.
Bowel diary and poo charts
As a busy parent, I can't accurately know all of my family's bowel habits! I imagine this may be the case with a fair few other parents as well. Collecting this type of information along with stool consistency can be really useful to look at together in clinic, and so I will often recommend this 'homework' exercise be used. There are various bowel diaries available but one really fun one is here.
For more information about poo please have a look at this excellent poo-torial from Guts UK, a charity that funds research into all things Gastrointestinal including the pancreas.
If
you have worries or concerns about your child's poo or other tummy troubles:
Please don't hesitate to be in touch. If you're looking to discuss things further or want to arrange to have a thorough paediatric gastroenterology assessment then please have a look at the main website for more information regarding Kids Gastro Care clinics and how to book an appointment with me.
Feedback about this post or other KGC output
(for want of a better word!)
Feel free to leave a comment here, or via the Kids Gastro Care Facebook page
or send me an email here.
As a newbie at this (blogging not paeds gastro!) I would love to have your feedback about this article or other posts on the blog, the website or Facebook page.
Much Ado about Poo
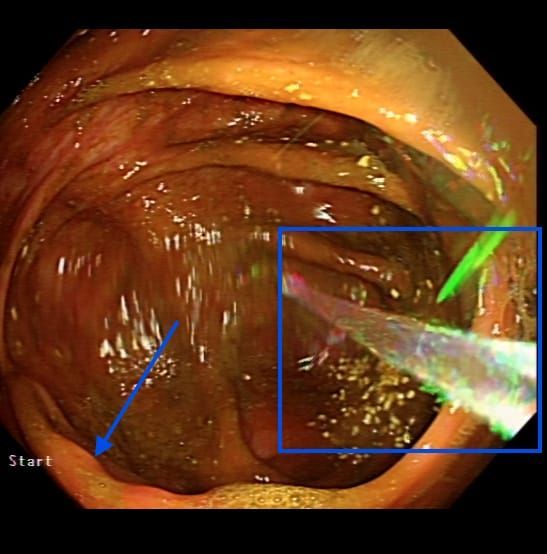
Bowel preparation plays a key role in your child having a successful paediatric colonoscopy
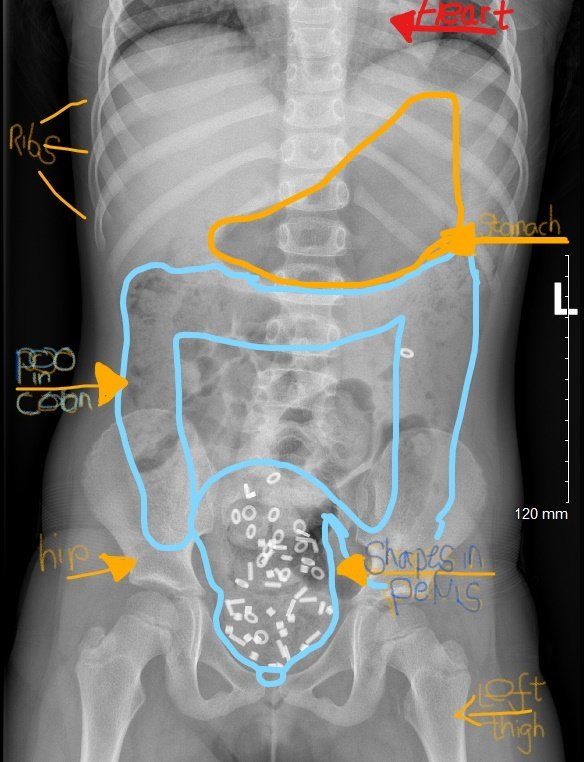
Constipation in children is a very common situation that I come across in my Kids Gastro Care clinics. The research literature often quotes a stat that up to 25 % of visits to a paediatric gastroenterologist are about constipation. Here I will discuss in some more detail, just one particular aspect of constipation in children, that of faecal incontinence or poo accidents. It is commonly associated with faecal impaction. For more on the diagnosis and management of constipation in children please click here. Being a 'poo doctor' I have become very used to talking about all aspects of bowel function and poo every day - just ask my kids! This isn't always the case for many others. There is still a great deal of stigma attached to poo problems in children and adults of all ages. One such area is around Poo accidents in children. Also called soiling, encopresis and faecal incontinence, it is not often the first thing that families talk about when I meet them in my clinics. In fact it may only come up when I directly ask about them. Poo accidents can be a tremendous source of upset, embarrassment, as well as social awkwardness, isolation and shame. They can leave parents frustrated at times as it is difficult to understand how their child can not seem to control their bowel motions. Sometimes children are told that they're being lazy and it can be easy to blame the child for the situation. I have seen children who needed upward of 8 changes of underwear and clothes a day because of poo accidents. Schools often send children home when these accidents occur. What should be fun childhood social activities such as swimming and sleep overs are limited or even stopped all together for fear of the dreaded accident happening. In the majority of children with poo accidents, the most common reason for this to occur is constipation. In some there is no significant constipation. I won't go into detail about that situation here in this post, as other aspects of care, often with a psychological emphasis, need to be addressed in greater detail. When there is a significant build up of poo within the large intestine (colon) or 'poo factory' as I call it, this is known as faecal impaction . Often the build up occurs in the very last section of the colon called the rectum - a sort of holding area for poo before it is passed out of the body. The impacted faeces sits in the colon and builds up gradually over time becoming more and more firm. Newer poo can sometimes slide past this mass of older poo, and slip out unannounced, as an accident. Sometimes this can be mistaken for diarrhoea. The rectum becomes more and more stretched over time. The usually sensitive rectum, loses its ability to sense being filled up with new poo as it has been stretched beyond its usual dimensions. Accidents can occur at any time, often seemingly without the child even noticing. To add to an already difficult situation, and because of the close location of the stretched rectum to the bladder, wee accidents can also become a part of the problem. Often this situation isn't recognised for what it is until late in the journey. A crucial early step is understanding what has happened and explaining how it has developed, using a non-judgemental, no blame approach. This combined with the right type of laxative treatment then aims to clear out - or disimpact - the old mass of poo that's been sitting there probably for some time. Occasionally, a special type of x ray of the tummy, a so called shape study (colonic transit study) may be used to help clarify the situation and visually demonstrate the build up of poo. The X ray picture at the top of this blog post, shows an accumulation of shapes in a mass of faeces in the pelvis,. This is in the last part of the colon with a stretched rectum. Other parts of the colon are also loaded with poo. The sensation of needing to go is weakened by this stretch of the rectum and so accidents occur regularly. The good news is that often dramatic improvements can be made when the situation is recognised and then managed appropriately with disimpaction . I have seen children go from having multiple accidents each day to none overnight, with a simple intervention using laxatives to clear out the impacted rectum . Disimpaction can either involve taking several days of oral laxatives in increasing amounts , or as an alternative more direct way, using 2 or 3 days of laxatives administered rectally - using enemas. Occasionally a combined approach is useful. Once this crucial first step has taken place, then a regular schedule of laxatives is needed to keep the colon clear and prevent a further build up. I really feel it's time to break down these taboos around poo and get this issue more widely recognised and then treated properly. Talking about poo with a fun down to earth approach is a start. It is only poo after all... If you think your child may be experiencing issues similar to those I have mentioned in this post, please do have a look at the Kids Gastro Care website for more information about constipation in children . If they're having troubles with their bowel control and you'd like to discuss things in more detail in an appointment with me, then please don't hesitate to be in touch and give us a call . The ERIC website , run by ERIC -the Childrens Bowel and bladder charity- is a fantastic resource for families affected by these issues. Please do help support their amazing work if you can by making a donation. I recently posted about this on our Facebook page with a request for donations for ERIC.
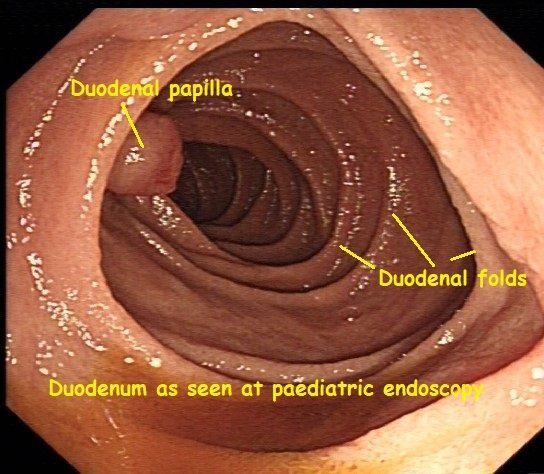
Every so often during my weekly paediatric endoscopy list, a striking image comes up on the screen, that makes me stop and reflect on the wonders of the human body. Here you can see a healthy-looking duodenum, from a recent paediatric endoscopy of the upper Gastrointestinal (GI) tract. This type of diagnostic endoscopy is also known as an Oesophago-gastro-duodenoscopy (OGD for short) or Gastroscopy. The duodenum, the first, and shortest part of the small intestine, derives its name from the Latin word duodeni. This refers to its length being approximately 12 finger-breadths. Partially digested stomach contents, in an acidic semi-fluid mass known as chyme, leave the stomach via the pylorus and enter the duodenum. Here further digestive processes take place. To help get your bearings with the image here, I'll explain a little more about some of the terminology and jargon used by an endoscopist. The central cavity of any hollow tube within the body is knows as its lumen. Having a good clear view of the lumen is essential during endoscopic procedures such as an OGD or colonoscopy. When trying to describe where a specific or noticeable feature or point of interest is during a procedure, and for ease of reference, endoscopists tend to compare the lumen of the bowel to a clock face. The protrusion visible at the 9 o'clock position, is the duodenal papilla. This is an important landmark seen during endoscopic procedures involving the upper gastrointestinal tract such as an OGD or ERCP. The latter is a specialised type of endoscopy used to look at the gall bladder, pancreas and their associated pipework (or ducts to be more formal). Digestive juices from the gallbladder and the pancreas are transported downstream via these sophisticated pipes (ducts) to just behind or upstream of the papilla. They are mixed together, then squirted through the papilla, into the lumen of the duodenum, to mix with the chyme and help with digestion. These digestive juices contain: - Bile salts that help emulsify fat - Pancreas enzymes to help digest food - Bicarbonate to neutralise the acidity of the chyme and protect the lining of the small intestine from acid damage. Anyone who has experienced the pain brought on by a gallstone lodged in some of the ducts draining the gallbladder or pancreas, can testify to the fact that it is almost impossible to stand during such an episode. Although less common in children, gallstones can occur and are associated with bowel conditions such as Crohn's disease. I couldn't help but think how fitting are the words of the blessing for good health "Asher Yatzar". "Blessed... who has formed man with wisdom and created within him many openings and hollow spaces. It is obvious and known before Your Seat of Honor, that if even one of them would be opened, or one of them would be sealed, it would be impossible [to survive and] to stand before You.” This is recited at times most of us take for granted, after going to the loo for a wee or a poo for example. There was just something about this image that made me recognise the importance of being grateful for simple things, such as all our pipes and tubes being in good working order. For more about common topics related to paediatric gastroenterology, digestion and endoscopy click here . And if you would like to meet to discuss a digestive problem your child has, please don't hesitate to be in touch by calling us or sending us an email .

How to diagnose Coeliac disease in children is an evolving process with some recent significant changes. Here Dr Daniel Crespi, a London based Paediatric gastroenterologist, goes through the different ways in which this common condition can present in children. He then takes you through the latest diagnostic routes available. These now include a so called Biopsy avoidance approach in a wider group of children than ever before. Having a specialist involved early on can help prevent experiencing some of the pitfalls in diagnosing this common condition.
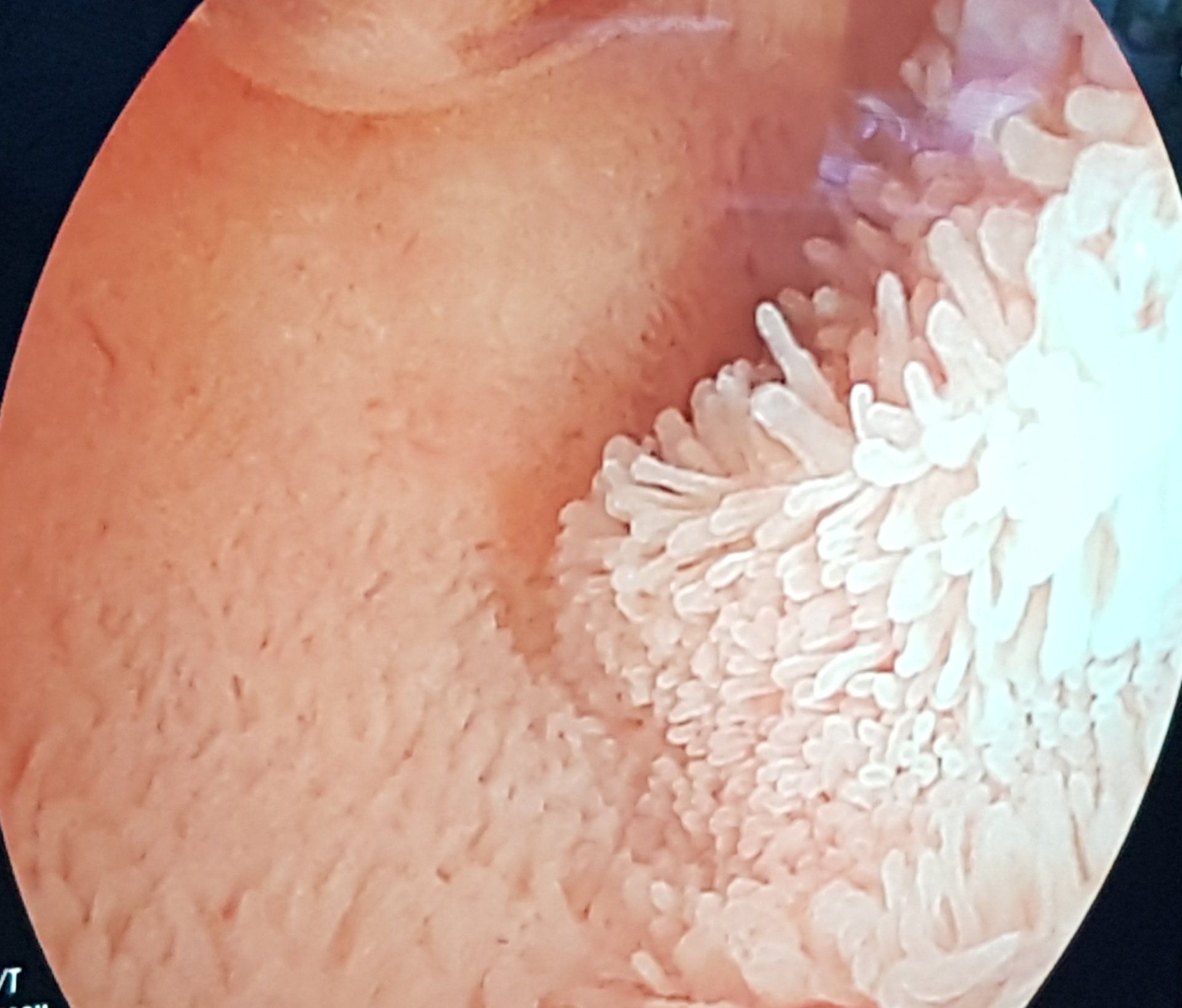
Every so often, I feel a sense of awe whilst at work. I came across this view during a specialised type of endoscopy (Double Balloon Enteroscopy or DBE) performed by a colleague, and I had that feeling again. Seeing a moving carpet of villi, the tiny finger like projections that coat the inner lining or mucosa of the small intestine in such detail, brought home to me the incredible workings of the human body, and how fortunate I am to be able to see this on a regular basis. Thousands upon thousands of these amazing structures help to hugely increase the surface area available for absorption of essential nutrients. including iron and vitamins. The small bowel can be affected by a variety of conditions that inflict damage to the villi. This impairs their ability to function so that one is at risk of malabsorption. Examples include Coeliac disease and Crohn's disease. Sometimes suspicion of the likely nature of the disease and it's involvement of the small intestine isn't enough. This is especially true when considering the use of potent medications that suppress the immune system, with the aim of healing the damaged areas. Having actual visual and biopsy proven evidence of involvement of this section of the GI tract can be crucial in deciding on the next steps in managing a condition. With most of its length, aside from the first and last few centimetres, being beyond the reach of standard upper and lower Gastrointestinal (GI) endoscopy, the small bowel has always been harder to investigate. Imaging using Barium with x rays is now rarely if ever used as other radiological techniques are available and also to avoid excessive radiation exposure especially in children. MRI of the small intestine gives a huge amount of information not only about the small bowel but also surrounding areas and organs. It is used in both children and adults. Ultrasound of the small intestine, in the right hands, can also give very useful information about the state of the small bowel particularly with regard to whether it is affected by inflammation in Crohn's disease. It is particularly useful in children as it avoids the sometimes claustrophobic feeling some can feel when in an MRI scanner as well as being faster and cheaper. Using Double Balloon Enteroscopy or DBE, it is possible to inspect the entire length of the lining of the small intestine. It allows the endoscopist to reach a lot further than a standard upper GI endoscopy or OGD does. The same is true of video capsule endoscopy (VCE), the miniaturised video camera within a swallowed pill, that takes thousands of images of the small intestine as it moves along it. In very simple terms, I think of the VCE as a reconnaissance of the area, scouting for anything abnormal. A form of window shopping, when I can only see the area of interest, however I can't sample what I see. With DBE one can both see and sample the lining with a biopsy and in some cases therapeutic techniques can be used. The VCE is often used as a screening investigation and then if needed, one can literally examine the depths of the small bowel with the DBE to obtain samples of tissue for examination under a microscope. The two techniques complement one another and along with other investigations, when put together like a jigsaw, help build up the bigger picture. Both techniques have their pros and cons of course and these are always discussed in detail before they are used. Carefully selecting the right test for the right patient is part of the challenge so as not to lead to any harm that could have been avoided. For more information and child friendly videos on endoscopy, have a look at the Useful resources page of the website.

Here Dr Daniel Crespi, a London based paediatric gastroenterologist, takes the reader on a short journey describing the way that these latest Inflammatory Bowel Disease Standards of care have been arrived at over several years.
Good article on the BBC website discussing some research from King's College London. We talk about constipation in the paediatric gastro and nurse -led constipation clinics but are we actually talking about the same thing that patients are when we discuss it. Patients and their doctors and nurses should all be on the same page when it comes to defining what constipation is.
As a 'poo' doctor I make no apologies for getting into the nitty gritty detail about bowel habits in consultations to make sure I get a good understanding of the situation from the patient perspective. It's only poo after all. Breaking down the taboo further. A good read for all of us.
https://www.bbc.co.uk/news/health-48528058
It's a phrase one often hears.. 'follow your gut feeling' but what is that all about? Intuition or 'gut feeling' is something we all feel at different times. Some researchers from Florida State University have found that gut feelings are part of a protective system helping us to avoid running into trouble. Powerful gut to brain signals have a significant effect on our emotions and decisions. This is something I often talk about with patients...how the gut and brain are hard wired to one another and constantly communicating. It's a fascinating area with lots of research going on. This so called gut-brain axis has a significant role to play in many symptoms and conditions that are commonly seen in a gastroenterology clinic and offers another angle when it comes to formulating a treatment strategy. You can read more about it in the article published in the journal Physiology in 2018 authors L Rinaman and J Maniscalco. More on this in future posts.
A fantastic 2 day course run by the team at the Royal London Hospital. It covered all aspects of Neurogastroenterology. Studies show that a large number of GI outpatient consultations revolve around conditions within this subspecialty of gastroenterology. Understanding the mechanisms behind the development of these conditions allows for a more personalised treatment plan incorporating a biopsychosocial approach. (Image from D.A Drossman, Rome III (3) process , Rome Foundation).